Pharmacology: Pharmacodynamics: Mechanism of action: Paliperidone palmitate, the active ingredient in Paliperidone palmitate (Invega Trinza), is a psychotropic agent belonging to the chemical class of benzisoxazole derivatives (atypical neuroleptic antipsychotic). Paliperidone palmitate (Invega Trinza) contains a racemic mixture of (+)- and (-)- paliperidone.
Paliperidone palmitate is hydrolyzed to paliperidone (see Toxicology: Non-Clinical Information as follows). Paliperidone is a centrally active dopamine D
2 antagonist with predominant serotonergic 5-HT
2A antagonistic activity. Paliperidone is also active as an antagonist at α
1 and α
2 adrenergic receptors and H
1 histaminergic receptors. Paliperidone has no affinity for cholinergic muscarinic or β
1- and β
2-adrenergic receptors. The pharmacological activity of the (+)- and (-)- paliperidone enantiomers is qualitatively and quantitatively similar.
The mechanism of action of paliperidone, as with other drugs having efficacy in schizophrenia, is unknown. It has been proposed that the therapeutic activity of paliperidone in schizophrenia is mediated through a combination of dopamine Type 2 (D
2) and serotonin Type 2 (5HT
2A) receptor antagonism. Antagonism at receptors other than D
2 and 5HT
2A may explain some of the other effects of paliperidone.
Effect on QT/QTc interval and cardiac electrophysiology: The effects of paliperidone on the QT interval were evaluated in a double-blind, active-controlled (moxifloxacin 400 mg single dose), multicenter Thorough QT study with oral paliperidone in adults with schizophrenia and schizoaffective disorder, and in four fixed-dose efficacy studies and one maintenance study of the 1-month paliperidone palmitate injectable product.
In the Thorough QT study (n = 141), the 8 mg dose of immediate-release oral paliperidone (n=50) showed a mean placebo-subtracted increase from baseline in QTcLD (QT interval corrected for heart rate using the population specified linear derived method) of 12.3 msec (90% CI: 8.9; 15.6) on day 8 at 1.5 hours post-dose. The mean steady-state peak plasma concentration for this 8 mg dose of paliperidone immediate release (C
max ss = 113 ng/mL) was approximately 2-fold the exposure with the maximum recommended 525 mg dose of Paliperidone palmitate (Invega Trinza) administered in the deltoid muscle (predicted median C
max ss = 56 ng/mL). In this same study, a 4 mg dose of the immediate-release oral formulation of paliperidone, for which C
max ss = 35 ng/mL, showed an increased placebo-subtracted QTcLD of 6.8 msec (90% CI: 3.6; 10.1) on day 2 at 1.5 hours post-dose.
In the four fixed-dose efficacy studies of the 1-month paliperidone palmitate injectable product, no subject had a change in QTcLD exceeding 60 msec and no subject had a QTcLD value of > 500 msec at any time point. In the maintenance study, no subject had a QTcLD change > 60 msec, and one subject had a QTcLD value of 507 msec (Bazett's QT corrected interval [QTcB] value of 483 msec); this latter subject also had a heart rate of 45 beats per minute.
In the long-term relapse prevention trial of Paliperidone palmitate (Invega Trinza) in subjects with schizophrenia, an increase in QTcLD exceeding 60 msec was observed in 1 subject (< 1%) in the open-label phase, no subject had an increase in QTcLD exceeding 60 msec after treatment with Paliperidone palmitate (Invega Trinza) in the double-blind phase, and no subject had a QTcLD value of > 480 msec at any point in the study.
Clinical efficacy: The efficacy of Paliperidone palmitate (Invega Trinza) for the treatment of schizophrenia in subjects who have been adequately treated for at least 4 months with the 1-month paliperidone palmitate injectable product was evaluated in a long-term double-blind, placebo-controlled relapse prevention/randomized withdrawal study and in a long-term double-blind, active-controlled noninferiority study.
Relapse prevention/randomized withdrawal study: Adult subjects who met DSM-IV-TR criteria for schizophrenia could enter the study with acute symptoms (if previously treated with oral antipsychotics) or be clinically stable (if treated with long-acting injectable antipsychotics [LAI]). All subjects who previously received oral antipsychotics received the paliperidone palmitate 1-month initiation regimen (deltoid injections of 234 mg and 156 mg one week apart), while those subjects switching from LAI medication were treated with the 1-month paliperidone palmitate injectable product in place of the next scheduled injection. Specifically: For subjects entering the study who were already being treated with the 1-month paliperidone palmitate injectable product, their dosing remained unchanged. Subjects who were currently receiving the 39 mg dose of 1-month paliperidone palmitate were not eligible to enroll in the study.
Subjects entering the study who were being treated with 25 mg, 37.5 mg, or 50 mg of Risperidone (Risperdal Consta) (risperidone long-acting injection) were switched to 78 mg, 117 mg, or 156 mg, respectively, of the 1-month paliperidone palmitate administered in the deltoid muscle.
Subjects entering the study who were being treated with any other LAI product were switched to 234 mg of the 1-month paliperidone palmitate administered in the deltoid muscle.
This study consisted of the following three treatment periods: A 17-week flexible-dose open-label period with the 1-month paliperidone palmitate (first part of a 29-week open-label stabilization phase). A total of 506 subjects entered this phase of the study. Dosing of the 1-month paliperidone palmitate was individualized based on symptom response, tolerability, and previous medication history. Specifically, the dose could be adjusted at the week 5 and 9 injections and the injection site could be deltoid or gluteal. The week 13 dose had to be the same as the week 9 dose. Subjects had to be clinically stable at the end of this period before receiving Paliperidone palmitate (Invega Trinza) at the week 17 visit. Clinical stability was defined as achieving a PANSS total score < 70 at week 17.
A 12-week open-label treatment period with Paliperidone palmitate (Invega Trinza) (second part of a 29-week open-label stabilization phase). A total of 379 subjects received a single dose of Paliperidone palmitate (Invega Trinza) which was a 3.5 multiple of the last dose of the 1-month paliperidone palmitate. Subjects had to remain clinically stable before entry into the next period (double-blind). Clinical stability was defined as achieving a PANSS total score < 70 and scores of ≤ 4 for PANSS items P1, P2, P3, P6, P7, G8, and G14 at the end of this 12-week period (week 29 of the study).
A variable length double-blind treatment period. In this period, 305 stabilized subjects were randomized 1:1 to continue treatment with Paliperidone palmitate (Invega Trinza) or placebo until relapse, early withdrawal, or the end of study. Subjects were randomized to the same dose of Paliperidone palmitate (Invega Trinza) they received during the open-label phase (i.e., 273 mg, 410 mg, 546 mg, or 819 mg) or to placebo administered every 12 weeks. The numbers (%) of subjects entering double-blind on each of the dose levels were 6 (4%) for 175 mg, 15 (9%) for 263 mg, 78 (49%) for 350 mg, and 61 (38%) for 525 mg.
The primary efficacy variable was time to first relapse. Relapse was pre-defined as emergence of one or more of the following: psychiatric hospitalization, ≥ 25% increase (if the baseline score was > 40) or a 10-point increase (if the baseline score was ≤ 40) in total PANSS score on two consecutive assessments, deliberate self-injury, violent behavior, suicidal/homicidal ideation, or a score of ≥ 5 (if the maximum baseline score was ≤ 3) or ≥ 6 (if the maximum baseline score was 4) on two consecutive assessments of the individual PANSS items P1 (Delusions), P2 (Conceptual disorganization), P3 (Hallucinatory behavior), P6 (Suspiciousness/persecution), P7 (Hostility), or G8 (Uncooperativeness).
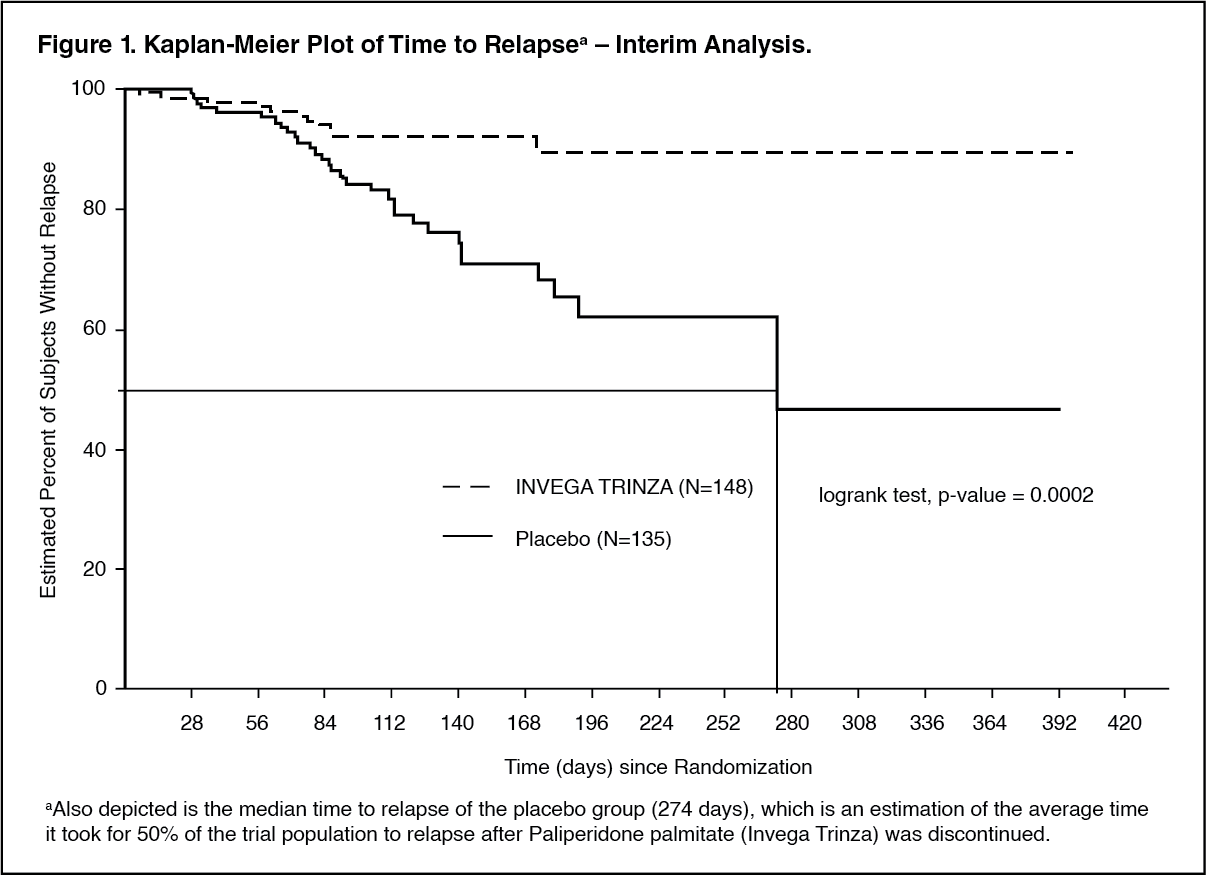
A pre-planned interim analysis showed a statistically significantly longer time to relapse in subjects treated with Paliperidone palmitate (Invega Trinza) compared to placebo, and the study was stopped early because efficacy was demonstrated. The most common reason for relapse observed across both treatment groups was increase in the PANSS total score value, followed by psychiatric hospitalization.
The mean (SD) duration of exposure during the double-blind phase was 150 (79) days in the placebo group and 175 (90) days in the Paliperidone palmitate (Invega Trinza) group. Twenty-three percent (23%) of subjects in the placebo group and 7.4% of subjects in the Paliperidone palmitate (Invega Trinza) group experienced a relapse event. The hazard ratio for relapse (placebo/Paliperidone palmitate (Invega Trinza)) was 3.45 (95% CI: 1.73, 6.88) indicating a 71% decrease in relapse risk with Paliperidone palmitate (Invega Trinza). There was a significant difference (p-value <0.001) between the treatment groups in favor of Paliperidone palmitate (Invega Trinza). A Kaplan-Meier plot of time to relapse by treatment group is shown in Figure 1. The median time to relapse (the time at which the cumulative survival function equals 0.5, or 50%) for subjects in the placebo group (274 days) was significantly shorter than for the Paliperidone palmitate (Invega Trinza) group (which could not be estimated as less than 15% of the remaining patients at any time during the trial experienced a relapse).
An examination of population subgroups did not reveal any clinically significant differences in responsiveness on the basis of gender, age, or race. (See Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Noninferiority study: In the noninferiority study, 1429 acutely ill subjects (baseline mean PANSS total score: 85.7) were enrolled into the open-label phase and treated with the 1-month paliperidone palmitate injectable product for 17 weeks. The dose could be adjusted (i.e., 50 mg, 75 mg, 100 mg, or 150 mg) at the week 5 and 9 injections and the injection site could be deltoid or gluteal. For subjects that met randomization criteria at weeks 14 and 17, 1016 were randomized in a 1:1 ratio to continue on monthly injections of the 1-month paliperidone palmitate injectable product or to switch to Paliperidone palmitate (Invega Trinza) with a 3.5 multiple of the week 9 and 13 dose of the 1-month paliperidone palmitate injectable product for 48 weeks. Subjects received Paliperidone palmitate (Invega Trinza) once every 3 months and received placebo injectable medication for the other months to maintain the blind.
The primary efficacy endpoint of the study was the percentage of subjects who had not relapsed at the end of the 48-week double-blind phase based on the Kaplan-Meier 48-week estimate (Paliperidone palmitate (Invega Trinza): 91.2%, 1-month paliperidone palmitate injectable product: 90.0%). The mean (SD) duration of exposure during the double-blind phase was 295 (88) days in the Paliperidone palmitate (Invega Trinza) group and 287 (96) days in the 1-month paliperidone palmitate injectable product group. The median time to relapse in either group could not be estimated due to low percentage of subjects with relapse. The difference (95% CI) between the treatment groups was 1.2% (-2.7%, 5.1%), meeting the pre-specified noninferiority criterion based on a margin of -15%. Thus, the Paliperidone palmitate (Invega Trinza) treatment group was noninferior to the 1-month paliperidone palmitate injectable product. Improvements in functioning, as measured by the Personal and Social Performance scale (PSP), which was observed during the open-label stabilization phase were maintained during the double-blind phase for both treatment groups. (See Figure 2.)
Click on icon to see table/diagram/image
The efficacy results were consistent across population subgroups (gender, age, and race) in both studies.
Pharmacokinetics: Absorption and distribution: Due to its extremely low water solubility, the 3-month formulation of paliperidone palmitate dissolves slowly after intramuscular injection before being hydrolyzed to paliperidone and absorbed into the systemic circulation. The release of the drug starts as early as day 1 and lasts for as long as 18 months.
The data presented in this paragraph are based on a population pharmacokinetic analysis. Following a single intramuscular dose of Paliperidone palmitate (Invega Trinza), the plasma concentrations of paliperidone gradually rise to reach maximum plasma concentrations at a median T
max of 30-33 days. Following intramuscular injection of Paliperidone palmitate (Invega Trinza) at doses of 175-525 mg in the deltoid muscle, on average, an 11-12% higher C
max was observed compared with injection in the gluteal muscle. The release profile and dosing regimen of Paliperidone palmitate (Invega Trinza) results in sustained therapeutic concentrations. The total exposure of paliperidone following Paliperidone palmitate (Invega Trinza) administration was dose-proportional over a 175-525 mg dose range, and approximately dose-proportional for C
max. The mean steady-state peak:trough ratio for a Paliperidone palmitate (Invega Trinza) dose was 1.6 following gluteal administration and 1.7 following deltoid administration. Following administration of Paliperidone palmitate (Invega Trinza), the apparent volume of distribution of paliperidone is 1960 L.
The plasma protein binding of racemic paliperidone is 74%.
Following administration of Paliperidone palmitate (Invega Trinza), the (+) and (-) enantiomers of paliperidone interconvert, reaching an AUC (+) to (-) ratio of approximately 1.7-1.8.
Metabolism and excretion: In a study with oral immediate-release
14C-paliperidone, one week following administration of a single oral dose of 1 mg immediate-release
14C-paliperidone, 59% of the dose was excreted unchanged into urine, indicating that paliperidone is not extensively metabolized in the liver. Approximately 80% of the administered radioactivity was recovered in urine and 11% in the feces. Four metabolic pathways have been identified
in vivo, none of which accounted for more than 10% of the dose: dealkylation, hydroxylation, dehydrogenation, and benzisoxazole scission. Although
in vitro studies suggested a role for CYP2D6 and CYP3A4 in the metabolism of paliperidone, there is no evidence
in vivo that these isozymes play a significant role in the metabolism of paliperidone. Population pharmacokinetics analyses indicated no discernible difference on the apparent clearance of paliperidone after administration of oral paliperidone between extensive metabolizers and poor metabolizers of CYP2D6 substrates.
In vitro studies in human liver microsomes showed that paliperidone does not substantially inhibit the metabolism of medicines metabolized by cytochrome P450 isozymes, including CYP1A2, CYP2A6, CYP2C8/9/10, CYP2D6, CYP2E1, CYP3A4, and CYP3A5.
In vitro studies have shown that paliperidone is a P-gp substrate and a weak inhibitor of P-gp at high concentrations. No
in vivo data are available and the clinical relevance is unknown.
Based on population pharmacokinetic analysis, the median apparent half-life of paliperidone following Paliperidone palmitate (Invega Trinza) administration over the dose range of 175-525 mg ranged from 84-95 days following deltoid injections and 118-139 days following gluteal injections.
Long-acting 3-month paliperidone palmitate injection versus other paliperidone formulations: Paliperidone palmitate (Invega Trinza) is designed to deliver paliperidone over a 3-month period, while 1-month paliperidone palmitate injection is administered on a monthly basis. Paliperidone palmitate (Invega Trinza), when administered at doses that are 3.5-fold higher than the corresponding dose of 1-month paliperidone palmitate injection, results in paliperidone exposures similar to those obtained with corresponding monthly doses of 1-month paliperidone palmitate injection and corresponding once daily doses of paliperidone extended-release tablets. The exposure range for Paliperidone palmitate (Invega Trinza) is encompassed within the exposure range for the approved dose strengths of paliperidone extended-release tablets.
Figure 3 presents the population predicted median pharmacokinetic profiles for paliperidone following Paliperidone palmitate (Invega Trinza) administration using the 350 mg and 525 mg doses compared to the administration of monthly injections of 100 mg and 150 mg 1-month paliperidone palmitate injection and to oral extended-release tablet administration (8 mg or 12 mg). Treatment with 1-month paliperidone palmitate injection for at least 4 months prior to initiating treatment with Paliperidone palmitate (Invega Trinza) resulted in maintenance of steady-state paliperidone plasma exposures. (See Figure 3.)
Click on icon to see table/diagram/image
Special populations: Elderly (65 years of age and older): No dosage adjustment is recommended based on age alone. However, dose adjustment may be required because of age-related decreases in creatinine clearance (see Renal impairment as follows and Dosage & Administration).
Renal impairment: Paliperidone palmitate (Invega Trinza) has not been systematically studied in patients with renal impairment. The disposition of a single oral dose of a paliperidone 3 mg extended-release tablet was studied in subjects with varying degrees of renal function. Elimination of paliperidone decreased with decreasing estimated creatinine clearance. Total clearance of paliperidone was reduced in subjects with impaired renal function by 32% on average in mild (CrCl = 50 to < 80 mL/min), 64% in moderate (CrCl = 30 to < 50 mL/min), and 71% in severe (CrCl = 10 to < 30 mL/min) renal impairment, corresponding to an average increase in exposure (AUC
inf) of 1.5, 2.6, and 4.8 fold, respectively, compared to healthy subjects. Based on a limited number of observations with Paliperidone palmitate (Invega Trinza) in subjects with mild renal impairment and pharmacokinetic simulations, the initiation and maintenance dose of 1-month paliperidone palmitate injection should be reduced in patients with mild renal impairment. Subjects can be transitioned over to Paliperidone palmitate (Invega Trinza) using the corresponding 3.5-multiple dose for mild renal impaired subjects. No additional dose reduction upon starting Paliperidone palmitate (Invega Trinza) is necessary. (See Dosage & Administration.)
Hepatic impairment: Paliperidone is not extensively metabolized in the liver. Although Paliperidone palmitate (Invega Trinza) was not studied in patients with hepatic impairment, no dose adjustment is required in patients with mild or moderate hepatic impairment. In a study with oral paliperidone in subjects with moderate hepatic impairment (Child-Pugh class B), the plasma concentrations of free paliperidone were similar to those of healthy subjects. Paliperidone has not been studied in patients with severe hepatic impairment.
Race: Population pharmacokinetics analysis of data from studies with oral paliperidone revealed no evidence of race-related differences in the pharmacokinetics of paliperidone following Paliperidone palmitate (Invega Trinza) administration.
Gender: No clinically significant differences were observed between men and women.
Smoking status: Based on
in vitro studies utilizing human liver enzymes, paliperidone is not a substrate for CYP1A2; smoking should, therefore, not have an effect on the pharmacokinetics of paliperidone. Consistent with these
in vitro results, population pharmacokinetic evaluation based on data from studies with the 1-month paliperidone injectable product has not revealed any differences between smokers and non-smokers.
Body Mass Index (BMI)/Body Weight: No dose adjustment is needed based on BMI. Lower C
max was observed in overweight and obese subjects. At apparent steady-state with Paliperidone palmitate (Invega Trinza), the trough concentrations were similar among normal, overweight, and obese subjects.
Toxicology: Non-Clinical Information: As with other drugs that antagonize dopamine D
2 receptors, intramuscularly-injected paliperidone palmitate, as well as orally-dosed paliperidone, elevated serum prolactin levels in repeat-dose toxicity studies.
In a 7-week juvenile toxicity study in rats with oral doses of paliperidone of 0.16, 0.63, and 2.5 mg/kg/day, which are 0.12, 0.5, and 1.8 times the maximum recommended human oral dose of 12 mg/day for adolescents on a mg/m
2 basis, no effects on growth, sexual maturation, and reproductive performance were observed. Oral doses up to 2.5 mg/kg/day did not impair neurobehavioral development in males and females, except for an effect on learning and memory in female rats treated at 2.5 mg/kg/day. This effect was not observed after discontinuation of treatment.
In a 40-week study in juvenile dogs treated with oral risperidone (which is extensively converted to paliperidone) at doses of 0.31, 1.25, and 5 mg/kg/day, sexual maturation was not adversely affected at 0.31 and 1.25 mg/kg/day. Long bone growth was not affected at 0.31 mg/kg/day; effects were observed at 1.25 and 5 mg/kg/day.
Carcinogenicity: The carcinogenic potential of intramuscularly injected paliperidone palmitate was assessed in rats. There was a statistically significant increase in mammary gland adenocarcinomas in female rats at 10, 30, and 60 mg/kg/month, which are 0.2, 0.6, and 1.1 times the maximum recommended Paliperidone palmitate (Invega Trinza) human dose of 525 mg on a mg/m
2 body surface area basis. Male rats showed a statistically significant increase in mammary gland adenomas and carcinomas at 30 and 60 mg/kg/month which is 1.3 and 2.5 times the maximum recommended human 525 mg dose of Paliperidone palmitate (Invega Trinza) on a mg/m
2 basis.
The carcinogenic potential of oral paliperidone, an active metabolite of risperidone, was assessed based on studies with risperidone conducted in mice and rats. Risperidone was administered at doses up to 10 mg/kg/day for 18 months to mice and for 25 months to rats. There were statistically significant increases in pituitary gland adenomas, endocrine pancreas adenomas, and mammary gland adenocarcinomas. An increase in mammary, pituitary, and endocrine pancreas tumors has been found in rodents after chronic administration of other antipsychotic drugs and is considered to be mediated by prolonged dopamine D
2 antagonism. The relevance of these tumor findings in rodents in terms of human risk is unknown.
Mutagenicity: No evidence of mutagenic potential for paliperidone was found in the Ames reverse mutation test, the mouse lymphoma assay, or the rat micronucleus test. Paliperidone palmitate showed no genotoxic properties in the Ames reverse mutation test or the mouse lymphoma assay.
Fertility: Although oral paliperidone treatment resulted in prolactin- and CNS-mediated effects, the fertility of male and female rats was not affected. At a maternally toxic dose, female rats showed a slightly lower number of live embryos.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image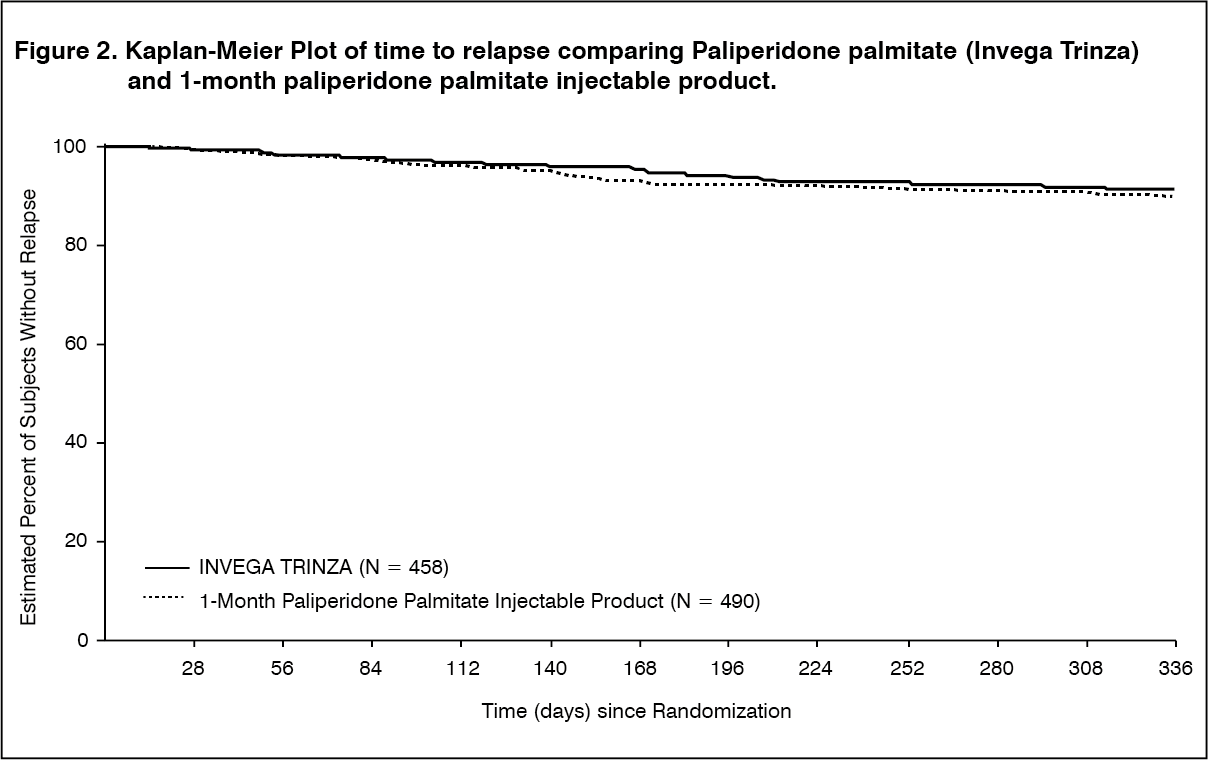 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image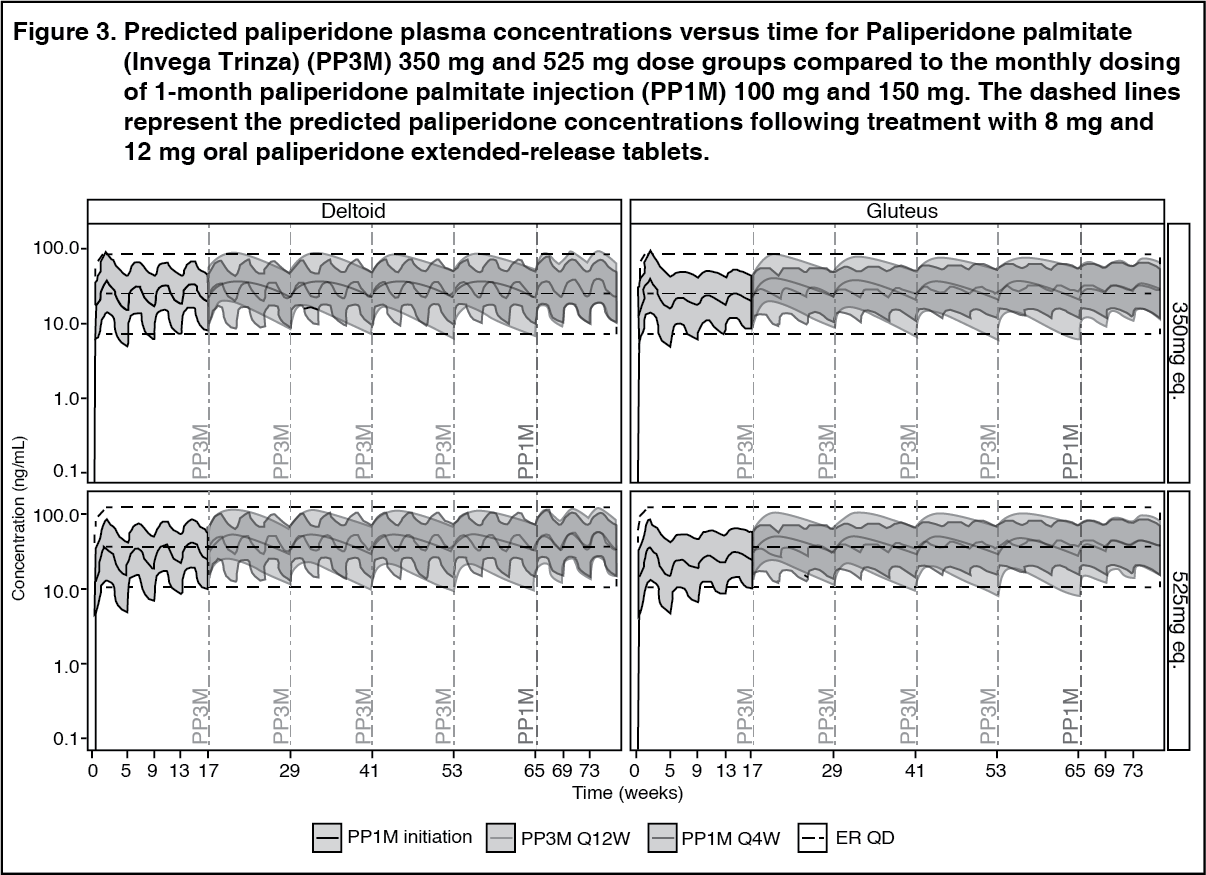 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image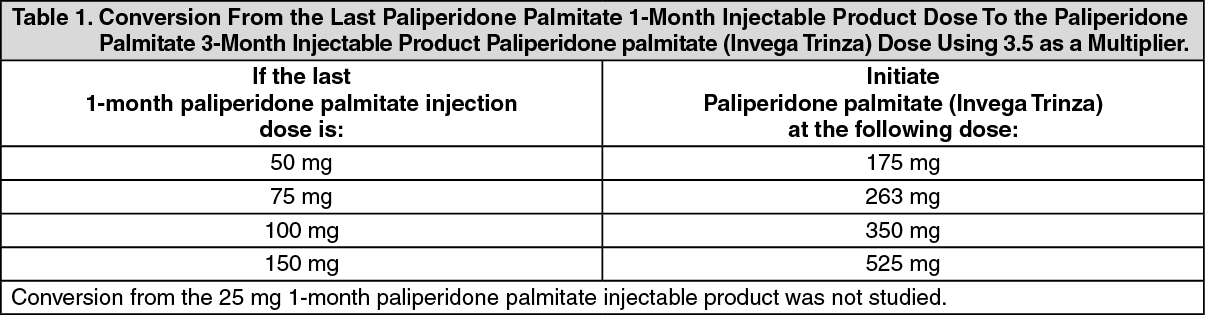 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image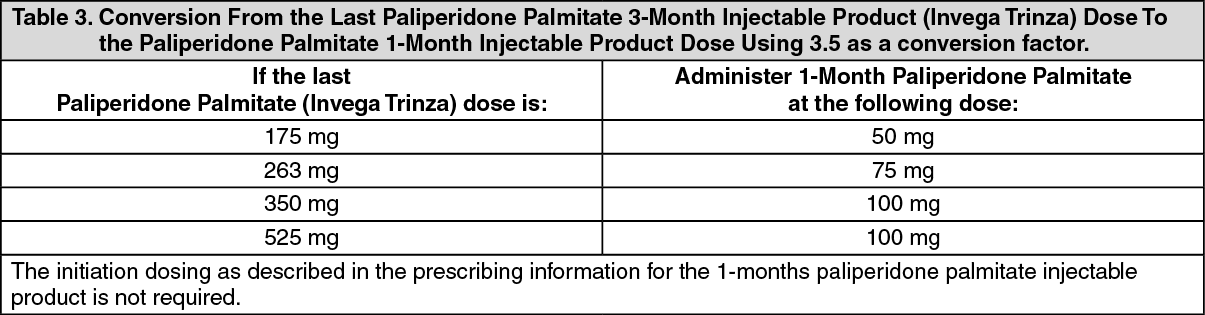 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image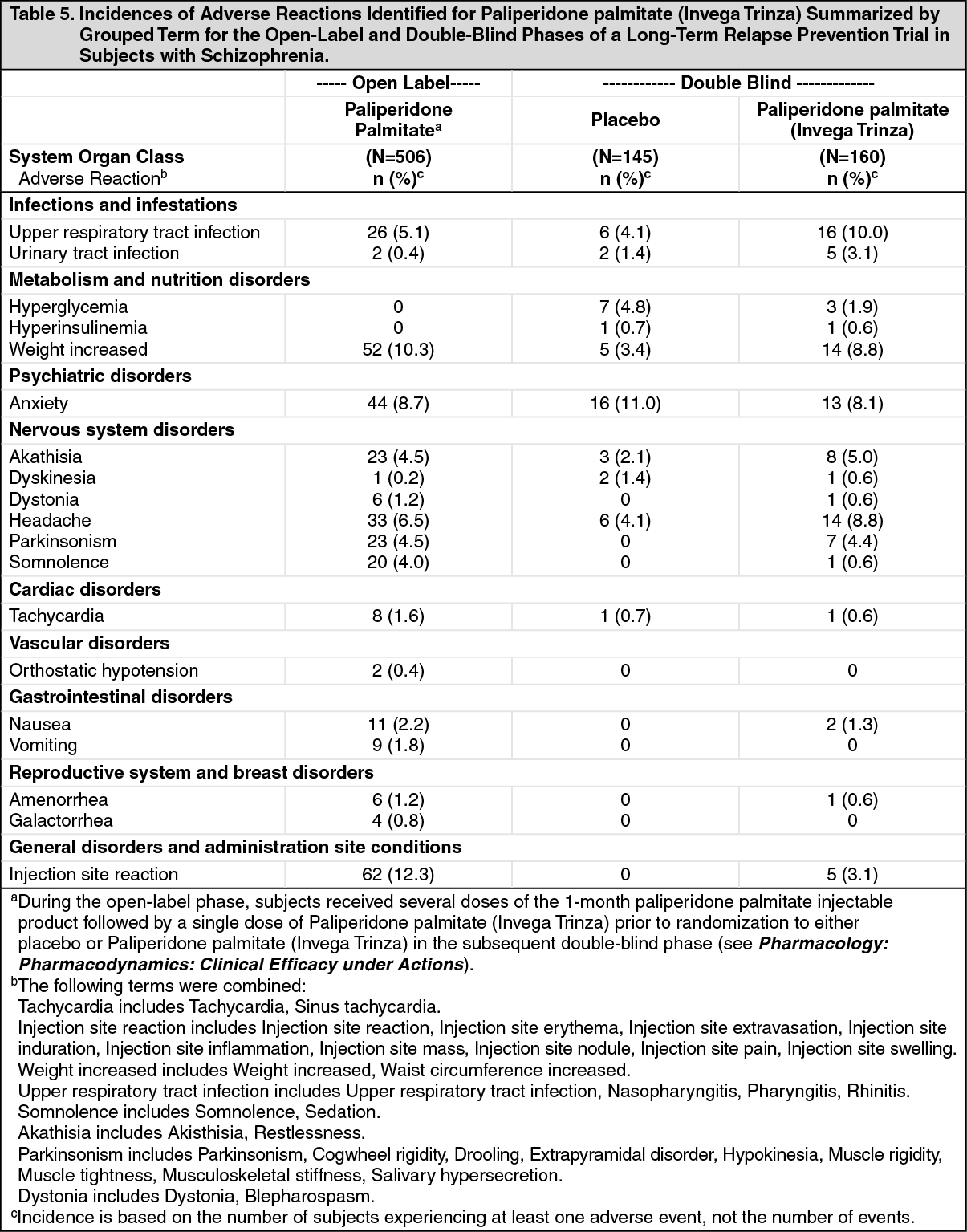 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out